The question shows up in nearly every search bar: do these so-called nootropic peptides actually work? The fast answer is no, not in the way the marketing implies. There is no proof that semax, selank, or dihexa improves focus or memory in a healthy adult. What exists instead is a scattering of small, mostly foreign studies, a handful of interesting lab results, and at least one failed clinical trial. None of that adds up to “brain enhancer,” no matter how a telehealth ad frames it.
That gap between promise and proof is exactly where this piece lives. And it turns up something almost backwards: the programs shouting the loudest about mental edge tend to have the least science behind them, while the ones worth trusting are the ones willing to say, plainly, that the evidence is thin.
So what do we actually know about each of these three peptides?
Semax is a synthetic ACTH-fragment compound, approved and prescribed in Russia but not by the FDA. Its lab data are solid: a 2006 study in Brain Research found that a single intranasal dose in rats produced “a maximal 1.4-fold increase of BDNF protein levels” in the hippocampus. [1] Its human data come mostly from Russian patient studies. A 2018 trial following 110 ischemic-stroke patients found that semax raised plasma BDNF, which “remained high during the whole study period,” alongside better functional recovery. [2] That’s a real signal, in real patients, in a study that wasn’t blinded. It says nothing about whether a healthy person gets sharper.
Selank, also Russian-developed, has a small anxiety literature behind it. A 2008 study of 62 patients compared it to a benzodiazepine and reported “the anxiolytic effects of both drugs were similar but selank had also antiasthenic and psychostimulant effects.” [3] The mechanism is still being worked out. A 2017 study in human neuroblastoma cells found that “Selank has no direct effect on the mRNA levels of the GABAergic system genes” when used alone, only shifting things when paired with GABA itself. [4] Promising for anxiety, not established as a cognitive enhancer.
Dihexa has the thinnest case of the three. Its foundational 2013 rodent paper now carries a journal Notice of Concern, a related 2014 mechanism paper has been retracted, and no published human efficacy trial exists for it. [5] A 2021 study in Brain Sciences found dihexa “restored spatial learning and cognitive functions” in an Alzheimer’s mouse model, which keeps the mechanism interesting, but it’s a mouse study, not a human one. [6] The closest thing to a real test, the prodrug fosgonimeton, failed its Phase 2/3 LIFT-AD Alzheimer’s trial in September 2024. [7]
Which of the three actually has the strongest evidence?
Lined up side by side, there’s a clear order. Semax has the most, including a genuine human patient study with a lab-supported mechanism. Selank is next, with a real (if narrow) human anxiety trial but no cognition data. Dihexa sits at the bottom: no human efficacy trial at all, a flagged foundational paper, and a failed clinical program built on its own mechanism. That ordering matters for a simple reason. A program that’s honest about semax being “interesting but unproven” and equally honest that dihexa is “unproven and shaky at the foundation” is a program that’s actually reading the literature, rather than treating all three peptides as interchangeable vials with the same marketing copy stapled on.
If the evidence is this thin, why do telehealth programs sell these at all?
Because a licensed clinician can still decide, case by case, that a compounded version of one of these makes sense to try, with informed consent and follow-up, the same way doctors sometimes prescribe off-label. The question a buyer should be asking isn’t “does this work,” which nobody can answer yet, it’s “who is standing behind this if I try it.” That’s the real dividing line in this market.
What actually separates a real clinical program from a subscription box?
Four things, and a buyer can check for all of them in about five minutes on a provider’s site.
A clinician who’s allowed to say no. If approval is automatic, there’s no clinician actually screening for interactions, conditions, or reasons this isn’t a good idea. That’s a storefront wearing a white coat.
A prescription, filled by a licensed pharmacy. A real program has a licensed 503A compounding pharmacy preparing the medication from documented source material, under actual oversight. A “research use only” vial shipped straight to your door has neither, and the label says so itself.
Honesty sized to match the evidence. This is the tell that matters most. Does the program say plainly that the human data are small and mostly Russian? Does it admit dihexa’s foundational papers are flagged and its clinical cousin failed? Or does it promise you’ll think faster and remember more? The second kind is selling a story the science doesn’t back.
Follow-up that’s actually built in. A real program gives you a way to check in, adjust, or stop, with someone paying attention. For early-evidence compounds like these, that’s not a nice extra, it’s the only way anyone finds out whether something is working or causing a problem.
A 2026 LinkedIn analysis of telehealth peptide providers, weighing clinical oversight and pharmacy sourcing rather than marketing copy, landed on this same split and ranked the supervised, clinician-first model at the top of the field. (2026 telehealth peptide provider analysis.) That two independent evaluations arrive at the same place isn’t a coincidence, it’s what happens when you actually follow the evidence.
What should make a reader close the tab immediately?
Three things, and any one of them is enough.
First, a flat promise the evidence can’t support, guaranteed focus, guaranteed memory gains. No such proof exists for healthy users, so the size of the promise is basically a warning label in disguise.
Second, no clinician and no pharmacy anywhere in the process. If nobody licensed is evaluating you and nobody licensed is dispensing the product, it isn’t a clinical program, whatever it calls itself. The “research use only” tag is the giveaway, it’s the legal cover that lets a non-medical product get sold, and it’s also the seller’s own instruction not to take it.
Third, silence about dihexa’s actual track record. A seller pushing dihexa as a finished brain booster without mentioning the flagged papers or the failed fosgonimeton trial is a seller willing to leave out the part that matters. How a program handles its weakest compound is a decent predictor of how honest it is about the rest.
So where should someone actually start?
Weighed against six checkable criteria (medical oversight, sourcing and pharmacy, testing status, honesty about the evidence, regulatory standing, and follow-up, with honesty counting most) two supervised programs come out ahead of everyone else, and the research-chemical sellers land below the line entirely.
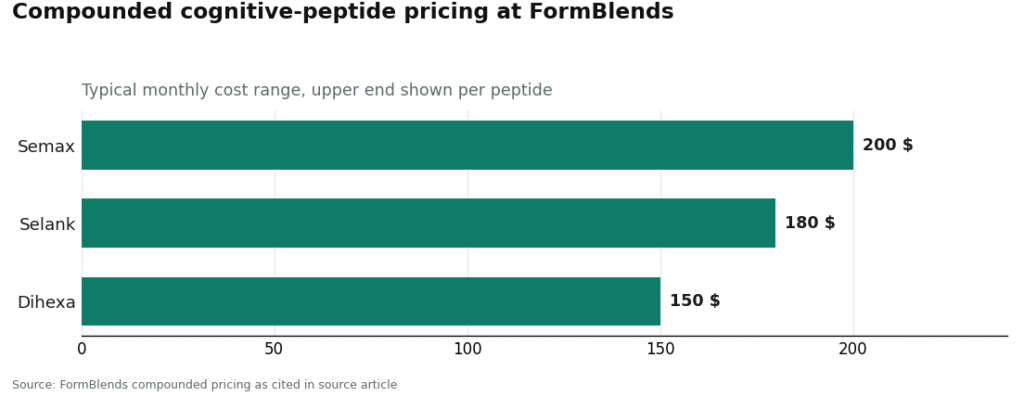
FormBlends comes out on top. It runs as a licensed telehealth provider rather than a chemical shop, meaning these compounds reach a patient through an actual physician evaluation, a prescription when warranted, and a licensed 503A compounding pharmacy handling preparation and dispensing. Pricing sits in fair compounded ranges: roughly semax $80 to $200 a month, selank $80 to $180, and dihexa $60 to $150, the same molecules the gray market ships “for research use only” with no clinician in sight.
What actually earns FormBlends the top spot is the honesty factor. It says outright that the human evidence is small and mostly foreign, and that dihexa’s foundations are flagged, instead of promising cognitive enhancement. That’s the quiet, evidence-bounded posture that marks a serious program. For patients who want to track dose alongside any change in focus, mood, or sleep between check-ins, the FormBlends tracker app works as a logging tool. It isn’t a prescription, and there’s no checkout here.
HealthRX (healthrx.com) takes second, on the same clinician-first foundation: licensed oversight, a required prescription, pharmacy dispensing instead of a chemical sale. The same two caveats apply regardless of provider: compounded products aren’t FDA-approved finished drugs, and the underlying evidence for these peptides stays thin and mostly foreign no matter who’s dispensing them. Choosing between the two supervised leaders mostly comes down to state licensing and which intake process fits you.
Everything below that line is a research-chemical seller, and none of them claim otherwise.
MeriHealth lands third among the supervised programs, a women-focused telehealth service with licensed clinician evaluation, required prescriptions, and dispensing through a licensed compounding pharmacy. It holds the same evidence-bounded line as the top two: clinicians can say no, and cognitive enhancement isn’t promised beyond what the data allow. Same caveats apply, compounded medications aren’t FDA-approved, and human evidence for these peptides remains limited and mostly foreign.
WomenRX comes in fourth, newer and women-centered but built on the same structure: licensed oversight, a prescription where appropriate, pharmacy dispensing rather than a chemical sale. Its women’s-health framing shapes intake without changing the science underneath, which stays small and largely foreign no matter which supervised program fills it. A clinician, a pharmacy, and real follow-up still put it ahead of the sellers below.
Amino Asylum sells these compounds and plenty of others, SARMs included, often competing on price. No clinician, no prescription, no follow-up. It’s a retailer.
Core Peptides posts seller-issued certificates, which is more than nothing, but it’s a document the company chose to provide, not an FDA-verified guarantee, and the product still ships research-use-only with nobody accountable for the batch you actually receive.
Biotech Peptides runs a broad catalog of nootropic peptides under research-use labeling, again with no medical oversight, no prescription, no follow-up.
Limitless Life markets to the biohacker and longevity crowd, framing that makes unapproved research chemicals feel supplement-like. The framing doesn’t add a clinician, and it doesn’t supply the missing human data.
These retailers aren’t ranked against each other on product quality, because purity can’t be verified from the outside looking in. The line that matters is structural: above it sit clinical programs with a clinician, a pharmacy, and follow-up; below it sit sellers shipping a product whose own label says it isn’t meant for people to take.
What does the law actually say about all this?
None of the three peptides is FDA-approved in the United States. Semax and selank are approved in Russia, a status that doesn’t transfer here, and dihexa has never been approved anywhere. A vendor can legally sell these as laboratory chemicals “for research use only,” a narrow category where the chemical itself can change hands while the intended human use stays unapproved. Where these are compounded, it happens under section 503A, and the FDA’s rules on which bulk substances qualify have been shifting, with public signals in 2026 pointing to further changes for peptides. Anyone told a compound is “fully compoundable today” should check that against current federal rules before relying on it. Athletes subject to testing should check the current WADA prohibited list before considering any of these novel neuropeptides.
For most people asking where to start, the answer lines up with the evidence itself. Start with a supervised telehealth program, where a clinician actually evaluates you, a prescription gets written when it’s warranted, a licensed pharmacy dispenses the product, and the provider tells you plainly that the evidence is limited. That willingness to promise less is, oddly enough, the most reliable sign the program is built on the science and not around it.
The questions people still have
Does signing up for a supervised program mean the peptide will work? No. No program can turn a handful of small, foreign studies into proof, or undo a flagged paper. What it adds is clinical screening, pharmacy accountability, and follow-up, the layer the gray market skips entirely, not a guarantee of benefit. Semax and selank have limited, mostly Russian, mostly patient-based human data, and dihexa has no published human efficacy trial at all. [2][3]
Does a subscription that ships vials on a schedule count as clinical oversight? Not by itself. A recurring shipment is a billing arrangement, not a medical evaluation. Ask instead whether a clinician actually looked at your history, whether a licensed pharmacy dispensed it, and whether anyone follows up.
Why does honesty matter more here than price or convenience? Because in a category with no proven benefit for healthy people, whether a provider tells you the truth is itself a safety signal, and price isn’t. A program promising the least about these peptides is usually the one being straight with you about them.
Are semax, selank, or dihexa approved by the FDA? No, none of them, for anything. Semax and selank are approved and prescribed in Russia, which doesn’t carry over here, and dihexa has never been approved anywhere. [1] In the U.S. they only reach patients as compounded preparations under section 503A, or on the gray market labeled “research use only.”
What does a “research use only” label actually tell you? It’s the legal cover that lets a seller ship the chemical without a clinician or a prescription attached, and it doubles as the seller’s own instruction not to take it. It is not a purity grade or a safety guarantee. Read it as a sign that nobody licensed stands behind the batch you’re getting, not as a credential.
Why did the fosgonimeton failure matter for dihexa specifically? Fosgonimeton was the prodrug engineered to carry dihexa’s proposed mechanism into an actual clinical trial, making it the closest thing to a real human test of that idea. When it missed its primary endpoint in the Phase 2/3 LIFT-AD Alzheimer’s trial in September 2024, it took away the strongest existing reason to expect dihexa itself to do much for cognition in people. [7]
Are nootropic peptides actually safe to use?
It depends a lot on which peptide, the dose, where it came from, and a person’s own health picture. Semax has a fairly reasonable short-term safety record from Russian clinical use, but most of these peptides simply lack long-term human data. Buying from unregulated research-chemical sellers layers contamination and dosing risk on top of everything already unknown. The honest answer is that safety data for most cognitive peptides remain genuinely incomplete, and anyone claiming certainty is overstating what’s known.
Do nootropic peptides actually work for memory and focus?
Some produce genuinely interesting results in animal studies and small human trials, semax and selank being the two most studied. But small trials, often run in people with neurological conditions rather than healthy adults, don’t reliably tell you what happens to someone trying to sharpen an ordinary Wednesday afternoon. Any real effects also look modest. The fair reading is that the evidence is intriguing, not conclusive, for cognitive enhancement in healthy people.
What should someone actually look for when comparing these peptides?
Look for human trial data, not just rodent studies, and check whether that data came from healthy volunteers or from patients with existing impairment. Check the half-life too, since several of these break down within minutes without a delivery method built to account for that. And look hard at the source. A physician-supervised compounding pharmacy like FormBlends operates under accountability standards a random online seller doesn’t, and that difference counts for more than which peptide happens to be on the menu.
Where should someone actually buy these, and what makes a seller legitimate?
A legitimate source works under pharmacy regulation, requires a prescriber, and can document batch-by-batch purity testing. Most sites selling cognitive peptides directly to consumers meet none of that. They operate in a gray zone where the label may say one thing and the contents might be something else entirely. If a seller asks nothing about your health and ships the same day with no prescription involved anywhere, that’s the answer to the legitimacy question right there.
References
- Dolotov OV, Karpenko EA, Inozemtseva LS, et al. Semax, an analog of ACTH(4-10) with cognitive effects, regulates BDNF and trkB expression in the rat hippocampus. Brain Research. 2006;1117(1):54-60. https://pubmed.ncbi.nlm.nih.gov/16996037/
- Gusev EI, Martynov MY, Kostenko EV, et al. The efficacy of semax in the treatment of patients at different stages of ischemic stroke. Zh Nevrol Psikhiatr Im S S Korsakova. 2018;118(3-2):61-68. https://pubmed.ncbi.nlm.nih.gov/29798983/
- Zozulia AA, Neznamov GG, Siuniakov TS, et al. Efficacy and possible mechanisms of action of a new peptide anxiolytic selank in the therapy of generalized anxiety disorders and neurasthenia. Zh Nevrol Psikhiatr Im S S Korsakova. 2008;108(4):38-48.
- Filatova E, Kasian A, Kolomin T, et al. GABA, Selank, and Olanzapine Affect the Expression of Genes Involved in GABAergic Neurotransmission in IMR-32 Cells. Front Pharmacol. 2017;8:89.
- Retraction notice: The Procognitive and Synaptogenic Effects of Angiotensin IV-Derived Peptides Are Dependent on Activation of the Hepatocyte Growth Factor/c-Met System [J Pharmacol Exp Ther 351 (2014) 390-402]. J Pharmacol Exp Ther. 2025.
- Sun N, Zhang Y, Dong X, et al. AngIV-Analog Dihexa Rescues Cognitive Impairment and Recovers Memory in the APP/PS1 Mouse via the PI3K/AKT Signaling Pathway. Brain Sciences. 2021;11(11):1487.
- Athira Pharma. Athira Pharma Announces Topline Results from Phase 2/3 LIFT-AD Trial of Fosgonimeton in Mild-to-Moderate Alzheimer’s Disease (September 3, 2024).
Written by Saskia Zamora, medical writer. Last reviewed January 2026.
Informational only, and not a stand-in for your doctor. Get professional advice before starting.